Systemic Sclerosis (SSc) has all sorts of impacts on the skin. Everyone with SSc will have skin changes of some kind. The type and severity of the skin involvement will vary, and is often related to the underlying subtype of SSc you may have. As a Dermatologist, helping patient’s understand and of course treat these, is one of my commitments.
If you haven’t read my page on “Scleroderma, Clearing up the Confusion”, it may be worth doing so.
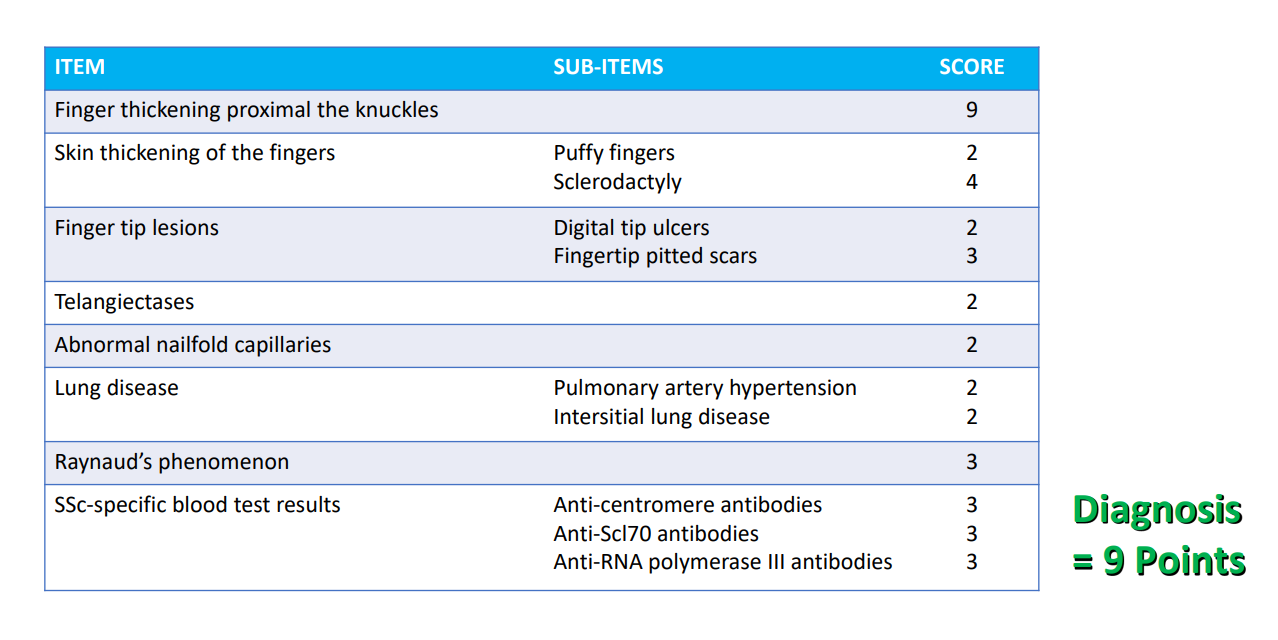
Key to SSc, is knowing that it is a very complex condition that affects the skin and many internal organs, including the lungs, gastrointestinal tract, kidneys and heart. There are specific criteria which have to be met before a diagnosis of SSc can be made. These include things such as the presence of:
- thickening and tightening of the skin on the fingers, called sclerodatyly = ‘hard fingers’
- certain specific antibodies in the blood which are not found in other conditions, such as anticentromere antibodies or anti-Scl70 antibodies
- abnormalities of the tiny blood vessels at the base of the nails or on the face
- fibrotic or vascular changes in the lungs which can be detected by breathing tests or lung scans.
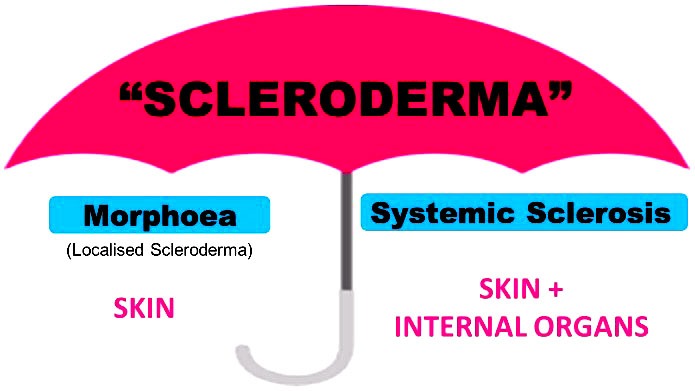
This is all very distinct to morphoea (aka Localised Scleroderma), which only affects the skin and tissues (such as the fat and fascia) that lie directly under the skin, with skin inflammation and tightness.
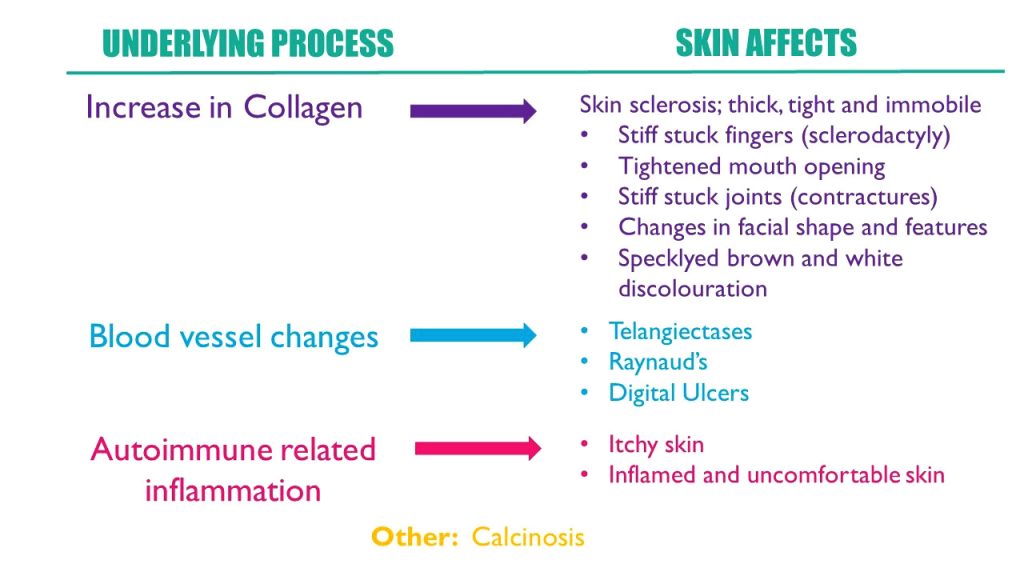
SSc is due to a complex combination of
- overproduction of collagen (‘fibrosis’ or ‘sclerosis’)
- inflammation caused by overactivity of the immune system (‘autoimmunity) and
- changes in the blood vessels,
which all result in the broad and varied symptoms and complications of the condition. These underlying changes are responsible for the different affects SSc has on the skin as well.
Many of these skin changes in SSc need separate consideration when it comes to managing symptoms and improving the skin’s function. So let’s discuss each of them here.
Skin tightening
The fundamental abnormality in SSc is the over production of collagen. This causes fibrosis. Fibrosis means that the connective tissues in the skin (and other organs such as the lungs), become thick, hard and tight. Almost 100% of those with SSc will have skin tightening (there is a very rare subtype of SSc which does not involve the skin called “systemic sclerosis sine scleroderma”). Affected skin is so tight and firm that it cannot be ‘pinched’ and it appears smooth and shiny.
The fingers / hands are most commonly involved in all subtypes of SSc. When the skin over the fingers becomes hard and immobile, the fingers get ‘locked’ in a bent position, and cannot straighten. We call this ‘sclerodactyly’. You can find plenty of photos of this on the internet. This has a huge impact on function and depending on severity can make simple daily tasks like writing, doing up buttons or holding a glass of water extremely difficult.
Similarly the toes can be affected.
If the skin tightness extends, it can involve the wrists, forearms and elbows. When skin over joints such as the wrists, ankles and elbows becomes tight and immobile, the joints contract and cannot be straightened, just like the fingers in sclerodactyly.
Skin tightness also often affects the face. This can change someone’s overall appearance and of course that can be very confronting and difficult for patients. In many ways, our faces are ‘us’. Our face is what we physically present to the world and how people recognise us. If that changes, it is naturally and understandably a really big and scary thing to happen. Face involvement can also lessen how wide the mouth can open, and this is called microstomia.
Treatment for skin tightness
Treating the skin tightness in SSc is the main goal of treatment of SSc. This is largely because often the excessive collagen deposition in the skin is also concurrently occurring in the lungs or elsewhere and so softening the tissues with treatment is key to halting the condition. Medications used for this aspect of treatment are often called ‘anti-fibrotics’. The most common is Mycophenolate Mofetil. You can read more about the treatments which can be tried for the inflammation and fibrosis in SSc on my Systemic Sclerosis Dermnet NZ page here.
General measures such as keeping warm, stretching exercises for joints to reduce the risk of worsening contractures and microstomia, and specifically-related physiotherapy can all be beneficial as well.
One of the most important aspects of treatment in SSc is starting it as early as possible. Having an early diagnosis and starting treatment early can prevent irreversible tissue damage and help lessen the long term impact the condition will have. Promisingly there is also a lot of progress being made nowadays to develop and test even more targeted and effective treatments for SSc.
After treatment
Down the track, once the skin tightness has been treated, and softened, there can be a relative loss of fat in the areas that were affected. When the skin is thickened by fibrosis, the extra collagen can become so thick that it extends down into the fat layer directly under the skin, and this means the fat is almost ‘gobbled up’ by all the extra fibrotic tissue.
On the face, this can result in wrinkles (sometimes called furrows) around the mouth, which can give an aged appearance. This is a difficult cosmetic problem. Fillers or autologous fat transfer are used (fat taken from somewhere else on the body and used to ‘fill’ these affected areas), but may be difficult to access.
Digital Ulcers
Breakdown of the skin, which we call an ulcer, can be caused by a few things in SSc:
- Reduced circulation, due to the effects of SSc on the blood vessels = Digital Ulcers
- Caclinosis; which can break down (see below)
- Trauma and poor skin healing; due to the skin being generally abnormal, tight and inflamed. Whilst this is obvious, doing all you can to avoid trauma can really help avoid problems in SSc; wear gloves, long sleeves and trousers, put a thick layer of a greasy moisturizer on – all these things can save your skin.
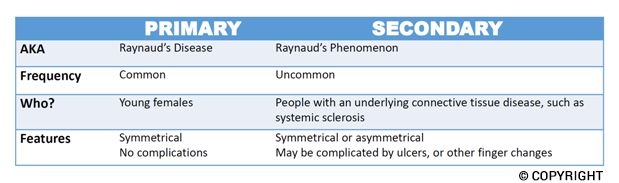
The term ‘digital ulcer’ usually refers to an ulcer on the fingers or toes which is a consequence of poor blood circulation in SSc. Digital ulcers tend to co-exist with severe Raynaud’s (cold hands or feet, with blue, white and/or red skin colour change. You can read more about Raynaud’s here. Raynaud’s and digital ulcers are signs that the blood flow to the peripheries (fingers and toes) is compromised.
The key to treatment is ideally to avoid such ulcers happening in the first place, if at all possible. There are lots of things you can do in that regard. The key is to keep warm.
- Do not smoke
- Avoid caffeine
- Avoid medications that constrict the blood vessels
- Keep your hands and feet as warm as possible; with double lined gloves, silver socks / thermal socks, heat pads for inside shoes and gloves.
- Avoid abrupt changes in temperature
- Avoid trauma
There are then lots of medical options to help the blood circulation to the fingers and toes. These include tablets and in severe cases, intravenous treatment with Iloprost. These treatments can help prevent digital ulcers and also promote healing of an ulcer if it has occurred.
Specific treatment for ulcers includes appropriate cleaning, dressings, avoiding and treating any infection with antibiotics, treating pain and any surrounding skin inflammation and dryness with moisturizers and/or steroid creams.
Telangiectases
Telangiectases (often called matt telangiectases) are small red spots on the skin produced by broken dilated superficial skin capillaries. In SSc these classically occur on the face, but can extend to the neck and chest, palms, or elsewhere.
These are a cosmetic concern, but they are of no other consequences.
Using green tinted makeup can often help camouflage the red spots and blend them into your background skin.
Vascular light or laser treatments can help, such as IPL or pulsed dye laser. Telengiectases in SSc are often stubborn and can recur, however laser treatment can result in a good cosmetic outcome in many patients, boosting confidence.
Itchy, dry and inflamed skin
Almost half of people with SSc will suffer from itchy skin during the course of their disease. Itch is just such an uncomfortable symptom. For some, it can be worse than pain. It impacts and infiltrates into every single aspect of your life and can feel impossible to escape. If persistent, itch really can be ‘enough to drive you mad’.
Very importantly, the skin in SSc is often dry and easily irritated, and that alone can go a long way to contributing to itch and general skin discomfort. Using a regular moisturizer and avoiding normal soaps can really help. I have more information about which moisturizer to use on the “FAQs in Scleroderma” page which you can check out here.
In SSc, itchy skin is generally a sign that the condition is active. It implies there is ongoing inflammatory changes in the skin, although not everyone with active SSc will have itchy skin.
Of course, itch can also be caused by a multitude of other causes too, unrelated to your SSc. It’s important you and your Dermatologist check for other possible contributing factors, like low Iron, or abnormal Thyroid Function. Other skin conditions can also co-exist with SSc, like eczema or rashes from viruses. All of this will be considered if you see a Dermatologist about your itchy skin.
Treating itchy skin in SSc can be tricky, but there are lots of options to try.
Calcinosis
Cutaneous calcinosis is the deposition of calcium in the skin. Calcinosis tends to occur over joints, such as on the fingers or elbows. However it can occur anywhere.
Calcium is very hard, and so when it deposits in the skin it produces firm hard lumps. These are usually small and just under the skin, but larger and deeper ‘chunks’ of calcium can occur. Sometimes the calcium can ‘pop through’ the skin as a white chalky material. In some cases this can cause ulceration, where the skin breaks down. However the biggest problem with calcinosis tends to be pain and discomfort.
Importantly, if calcinosis is not causing any pain or symptoms, it is perfectly safe to leave it there without any treatment.
Cutaneous calcinosis in SSc is notoriously challenging to treat and good studies into different treatments and their effectiveness are few and far between. Simple measures such as avoiding trauma, using protective gloves and ensuring the hands are kept warm (with good circulation) are important.
Prescription creams can sometimes help for smaller deposits; including extra strong topical steroid creams, and other specialised creams such as Sodium Thiosulfate. Prescription medications and procedures are often tried, and you can read about these in the Calcinosis section of my Systemic Sclerosis Dermnet NZ page.
Which treatments are applicable to you will depend on where your calcinosis is, how big the deposits are and how much trouble it causes you.
To finish up…
SSc is a complicated condition. I hope you’ve found some of this information useful.
To read more, you might find my Dermnet NZ page on Systemic Sclerosis or my review articles published in the Journal of the American Academy of Dermatology useful.
If you or a loved one have SSc and would like to book an appointment to see me, please contact my clinic.
Written by AProf Amanda Saracino
© 2023 AProf Amanda Saracino